Diagnosis
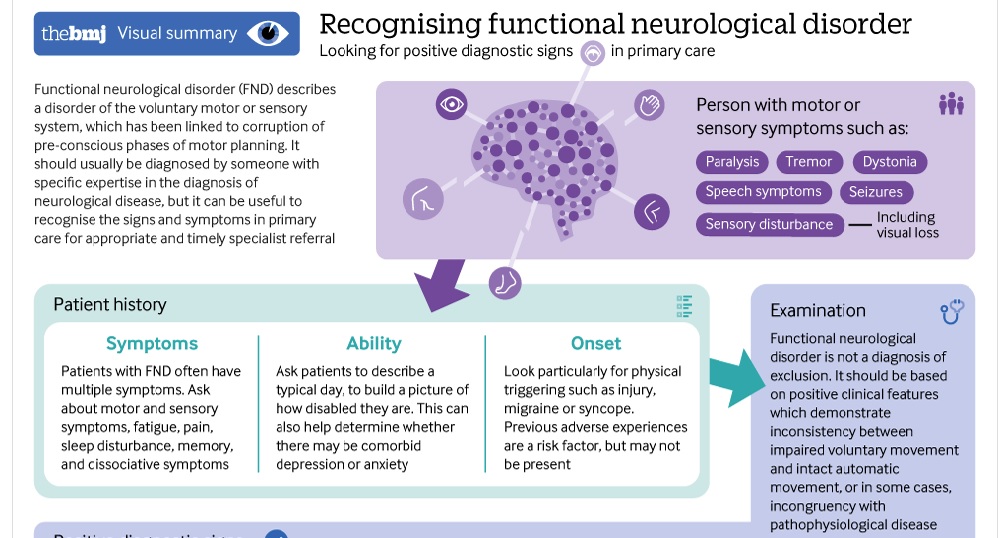
A diagnosis of Functional Neurological Disorder (FND) should be made by a Neurologist from positive signs/tests. It is not a diagnosis of exclusion, nor should symptoms be categorised as medically unexplained (MUS).
However, with currently no national NICE guidelines on how to diagnose and treat people with FND, in addition to the complexities surrounding the FND diagnosis in general and the lack of local funded services, inconsistencies in diagnosis and treatment continue to occur. This is unfair to both clinicians and people who receive the diagnosis. This has resulted in some people having good care and some not so good, with the most reporting that they have been given the FND diagnosis, been made to feel it is their fault, and directed to look it up online.
How a diagnosis of FND is delivered can have a positive or detrimental effect on the person receiving the diagnosis. Among other specialists in the field, Professor Mark Edwards runs an out-patient clinic in London specifically for those diagnosed with FND. In a publication[1] he discusses the importance of explaining to the patient what a diagnosis of FND means and what to do about it, and how failure to deliver the diagnosis correctly can impact on the therapeutic benefit of the consultation which is then lost. This in turn makes subsequent treatment more difficult.
Professor Edwards and colleagues also make it clear that focusing on the “how” rather than the “why” works well for many patients and their recovery.
Depending on symptoms presented the following tests/investigations may be used as part of diagnosing FND:
General medical examination, review of past history, and assessment of symptoms
It’s expected that this is performed at every initial appointment with the Neurologist. A medical examination is important to assess a person’s general health and wellbeing, and consider any other health problems/conditions that may be present given FND is not an overall diagnosis. Blood tests and other samples may be taken depending on symptoms. Other conditions that relate to the neurological symptoms the person is presenting with should be considered to avoid misdiagnosis. In addition; B12 and other deficiencies, side effects of medication, and emotional/mental health diagnosis’ should be considered.
CT (Computed Tomography) scan
An x-ray imaging test that provides detailed information on head injuries, stroke, brain tumours and other brain diseases. The examination involves you laying on a bed which slides into a ring shaped x-ray scanner.
MRI (Magnetic Resonance Imaging) scan
An imaging test that uses powerful magnets and radio waves to create pictures of the brain and surrounding nerve tissues, and used for the same purposes as a CT scan. As with a CT scan, you lay on a bed which slides in to the scanner, and creates more detailed pictures of tissues, organs and other structures within the body.
EMG (electromyography)/Nerve Conduction test
Test to measure and record electrical activity of the nerves and muscles.
EEG (Electroencephalogram)
A test used to assess electrical activity in the brain. It is performed by attaching sensors to the scalp to pick up electrical signals.
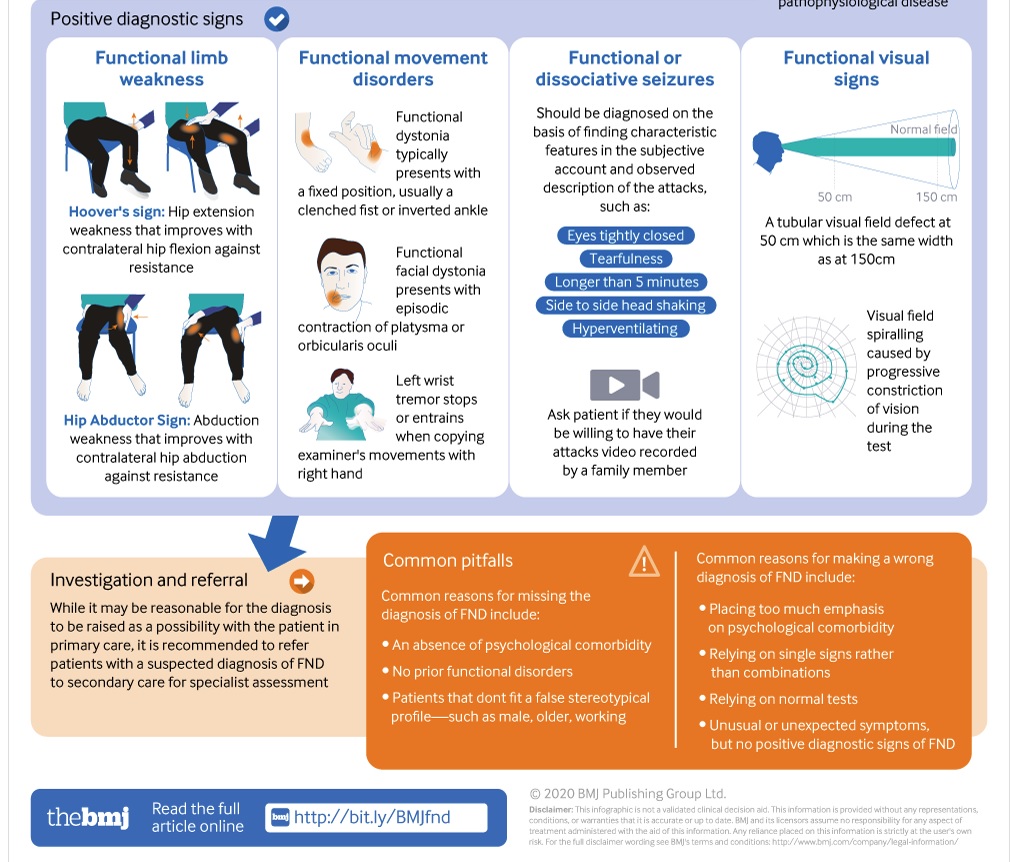
It is imperative that misdiagnosis is avoided at all costs, and below are a few common diagnostic errors that may occur – sourced from the consensus paper, A practical review of functional neurological disorder (FND) for the general physician which has been written by some of the leading specialists in the field.
Even if the diagnosis of FND is clear, always ask yourself whether it’s possible this is a patient with FND and another condition, possibly in a prodromal state (for example, functional tremor may occur in the early stages of Parkinson’s disease or functional/dissociative seizures may occur simultaneously with syncope or epilepsy).
There are many odd and unusual symptoms of other neurological conditions (such as geste antagoniste in dystonia, brief frontal lobe seizures with retained awareness and bicycling movements, ability to suppress movements in tics, and ability to self-induce epileptic seizures). The take home message is don’t diagnose FND because a presentation is unusual – there must be clear FND signs.
FND should not be diagnosed just because the patient has psychological comorbidity or recent stress. People with FND do tend to have, on average, more physical and psychological symptoms than equivalent disease controls. They are also more likely to have had adverse experiences both in childhood and more recently (odds ratio ∼2–4). However, all of these clinical features may occur in other disorders (such as multiple sclerosis or epilepsy) which are also associated with higher rates of psychiatric comorbidity. Migraine is a disorder also associated with increased adverse childhood experience in which neuroimaging is also usually normal. Conversely, the diagnosis of FND is often delayed in people without psychiatric comorbidity. FND seems to be especially rare in people with psychosis or where the presenting symptom is psychological.
Many neurological conditions may have normal structural imaging.
Incidental findings are common on brain magnetic resonance imaging (MRI), and disc disease is present in most people after the age of 40 years. Even EEG and cerebrospinal fluid oligoclonal bands can be false positive in some individuals.
To learn more about diagnostic signs and tests specifically for FND please refer to the diagram below and visit the neurosymptoms website
Stone J, Burton C, Carson A. Recognising and explaining functional neurological disorder BMJ 2020; 371 :m3745 doi:10.1136/bmj.m3745
Reference:
[1] Edwards, MJ. Functional neurological symptoms: welcome to the new normal Practical Neurology, 2016;16:2-3 doi:10.1136/practneurol-2015-00131
Share|Facebook
Share|Twitter
©FND Action. All Rights Reserved
Disclaimer | Privacy Policy
Registered Charity in England & Wales (1169554)
About Us | Facebook | Twitter
5a New Road Avenue
Chatham, Kent
ME4 6BB
Email: contact@fndaction.org.uk